Verified By: Dr. Mudit Khanna [MCh(UK), M.R.C.S(UK), M.S. Orthopaedics] Specialist in Joint Replacement, Arthroscopy and Trauma
Hip Dysplasia Treatment
When your child is diagnosed with hip dysplasia (also called developmental dysplasia of the hip, DDH), it’s normal to feel worried. The good news: most babies and children treated early go on to lead active, pain-free lives. India offers skilled paediatric orthopaedic teams, modern hospitals, and cost-effective care — all with strong support for international families.
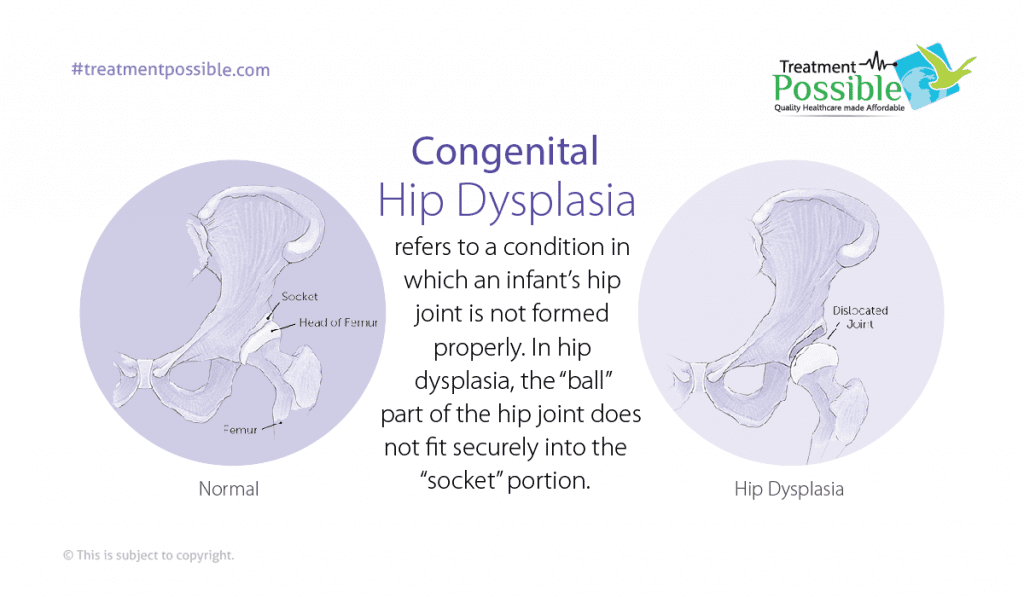
What is Congenital Hip Dysplasia?
Hip dysplasia is a condition in which an infant’s hip join is not formed properly. The “ball” at the top of the thigh bone (femoral head) doesn’t sit well in the hip socket (acetabulum). Due to this in newborns, the hip may be unstable, partially or completely dislocated, or the socket may be shallow. Early detection and treatment can help your child’s hip socket to develop properly so your child can walk, run and play normally later.
How do doctors screen and confirm DDH?
- Newborn physical exam: Doctors routinely check a newborn’s hips using the Barlow and Ortolani tests during the first hospital visit and follow-ups. If a hip sounds “clicky” or unstable, that triggers further testing.
- Ultrasound (sonography) for infants: If any abnormalities are found during the examination or risk factors are present (breech birth, family history, female sex), an ultrasound is the preferred test in babies under 6 months because it shows the cartilage and how the hip sits.
- X-rays for older infants/children: If the baby is 4–6 months old, X-rays become more useful as bones begin to ossify.
If hip dysplasia is identified in the first few months of life, it can be treated non-surgically, but a few cases may require surgery. When detected in early infancy, a non-surgical positioning device called a Pavlik harness may be used to keep a child’s hips flexed and abducted, correcting the alignment issues. Babies typically wear the harness for two to three months or until the hip issues are corrected. Afterwards, we follow patients for several years to make sure the child’s hips continue to function correctly.
Who is at higher risk?
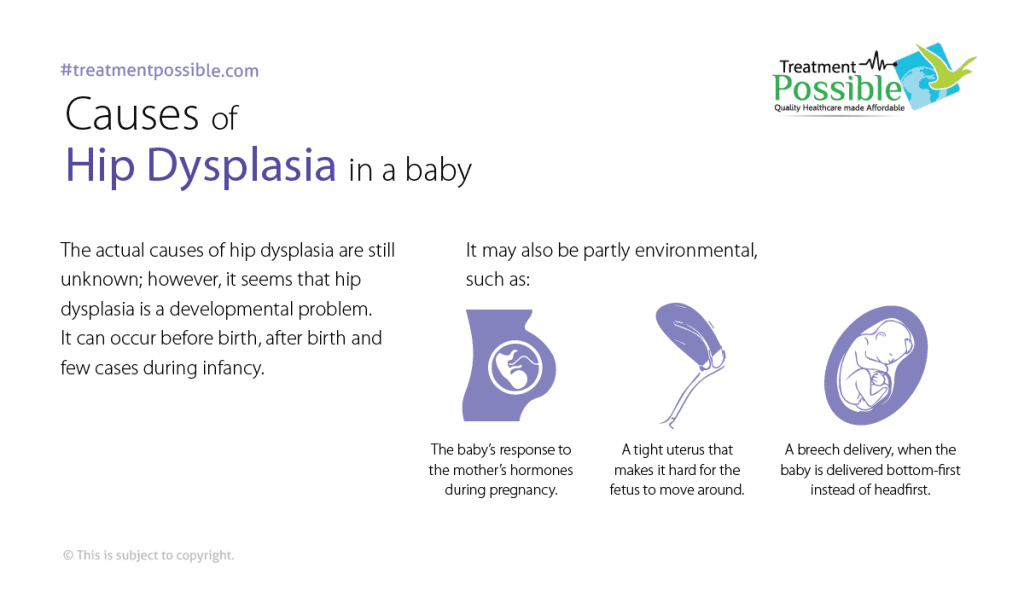
Hip dysplasia is a developmental problem. It can occur before birth, after birth and few cases during infancy.
- First-born babies are at higher risk because the uterus is small and there is limited room for the baby to move. That may affect how the hip develops.
- Orthopedic problems, such as clubfoot.
- Female babies (DDH is more common in girls)
- Babies who are born in the breech position (head up and feet down)
- A family history of hip dysplasia
- Very flexible ligaments
Knowing risk helps doctors decide who needs extra monitoring.
What are the Symptoms of Hip Dysplasia in a Baby?
The pain may start mild, but it can increase in severity and frequency over time. The pain associated with hip dysplasia is due to an abnormal amount of pressure placed on the rim of the socket. This pressure on the hip socket rim can lead to cartilage damage and eventually arthritis of the hip joint. The following are the common symptoms:
- The leg appears shorter on the side of the dislocated hip
- The leg on the side of the dislocated hip can turn outward
- The folds in the skin of the thigh or buttocks may appear uneven
- The space between the legs may look wider than normal
- Pain in the groin, side or back of hip joint
- Reduced range of movement in the hip joint
- Clicking or popping of the hip
Want more clarification about the condition & treatment?
Consult an Experienced Paediatric Orthopedic Specialist online for free.
How is Hip Dysplasia Treated?
Hip dysplasia is treated based on the age of the patient and the condition of the joint.
Infants (newborn to ~6 months)
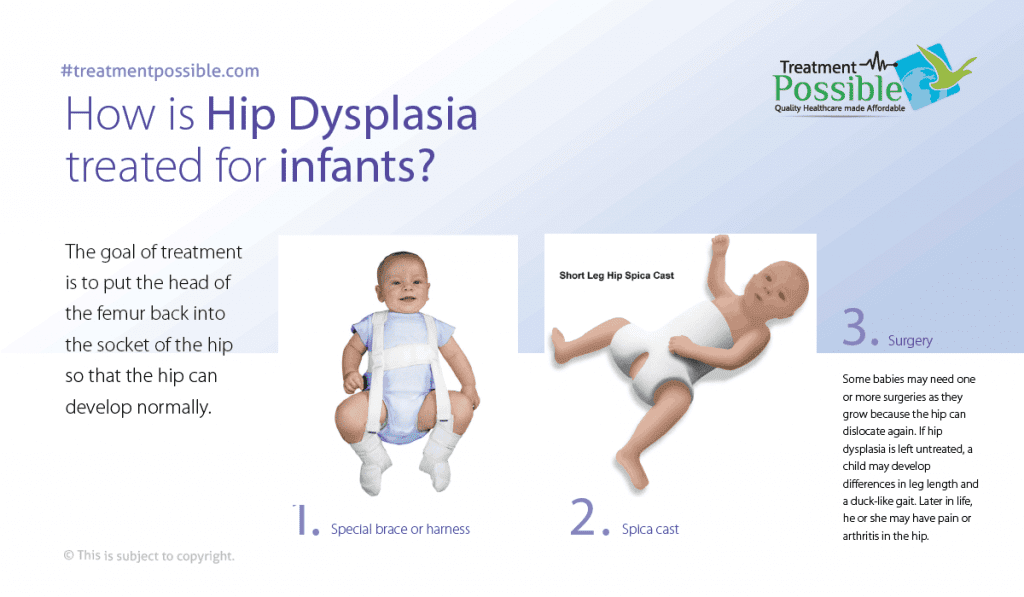
- Most common first step: Pavlik harness — A soft harness that holds the hips in a safe position while the socket molds around the ball. Parents usually keep it on full-time for several weeks to months, with regular checks and adjustments. In properly selected infants the harness succeeds in the majority of cases (many series report success in the ~80–85% range).
Infants (6–18 months)
- If the harness doesn’t work or diagnosis is later, children may need a Closed Reduction (a gentle procedure under anaesthesia to put the hip in place).
- Sometimes soft tissue can get in the way and a Open Reduction is performed, in which they will make a small incision to clear the path and place the hip joint in the correct position.
- Reduction is followed by a Spica Cast to hold the hip while it heals. After the cast is removed, your child will be given a special brace or physical therapy exercises to strengthen the muscles around the hip and in the legs.
Older children and adolescents
- Older children often need osteotomy procedures (bone realignment around the hip, such as pelvic or femoral osteotomy) to re-shape and stabilise the socket and ball. The goal is to prevent early arthritis and restore function. For adolescents and young adults with severe joint damage, hip-preserving surgery or even hip replacement may be considered.
- Periacetabular Osteotomy (PAO) – A hip-preserving orthopedic surgery in which the pelvis opened up and 4 cuts are made in the pelvis bone carefully to rotate the acetabulum. The goal of this surgery is to reorient the acetabulum to provide better coverage of the femoral head and to lessen the abnormal forces on the rim of the acetabulum. This reduces a patient’s pain and also decreases the chances of the patient developing arthritis.
Some babies may need one or more surgeries as they grow because the hip can dislocate again. If hip dysplasia is left untreated, a child may develop differences in leg length and a duck-like gait. Later in life, he or she may have pain or arthritis in the hip.
Summary of Hip Dysplasia in Children:
- Hip dysplasia in children is a health problem of the hip joint. The hip socket is shallow. This allows the head of the femur to dislocate, slipping in and out of the socket.
- Hip dysplasia is present at birth. It may be caused by genetic problems and environmental factors.
- A baby with Hip dysplasia may have one leg that looks shorter than the other.
- Newborns will be screened for Hip dysplasia before they leave the hospital.
- Treatment includes a Pavlik harness, casting, closed reduction or osteotomy.
What is the cost of treatment for Hip Dysplasia?
Typical cost ballpark (India): USD $5,000 – $7,000 for most infant/child DDH procedures (50% – 60% cheaper than other countries like US); complex osteotomy or revision cases may be higher. Final quote depends on exact procedure, hospital class and length of stay.
The cost includes: Visa assistance, airport transfers, accommodation, surgeon fees, anaesthesia, hospital bed charges, operating room, imaging, lab tests, post-op medicines, basic physiotherapy and a clear plan for follow-up.
Why do families choose India for DDH care (international patients)
Practical travel & care logistics for parents (what you’ll want to plan)
Next steps — How does Treatment Possible help you?
Send us your child’s latest reports and birth history — we’ll schedule an online appointment with a paediatric specialist and a transparent treatment plan so you can compare options with confidence.
Case Review
Arrange a free online case review with a paediatric orthopaedic specialist in India.
Cost Estimate
Provide detailed cost estimates from multiple accredited hospitals.
Coordinated Care
We arrange your medical visa, airport pickups, hospital admission, appointments, accommodation and telemedicine follow-up after you return home.